
")
")


Welcome to Janssen CarePath
VELETRI® (epoprostenol)
Main Menu
Downloadable Forms

- Janssen CarePath Resource Guide
 A comprehensive summary of support tools for your office to help patients start and stay on treatment.
A comprehensive summary of support tools for your office to help patients start and stay on treatment. - Patient Authorization FormA form for patients to allow their providers, insurers, and Janssen to share health information about them.
Patient Authorization Form (en español) - Patient Authorization Form (en español)A form for patients to allow their providers, insurers, and Janssen to share health information about them.
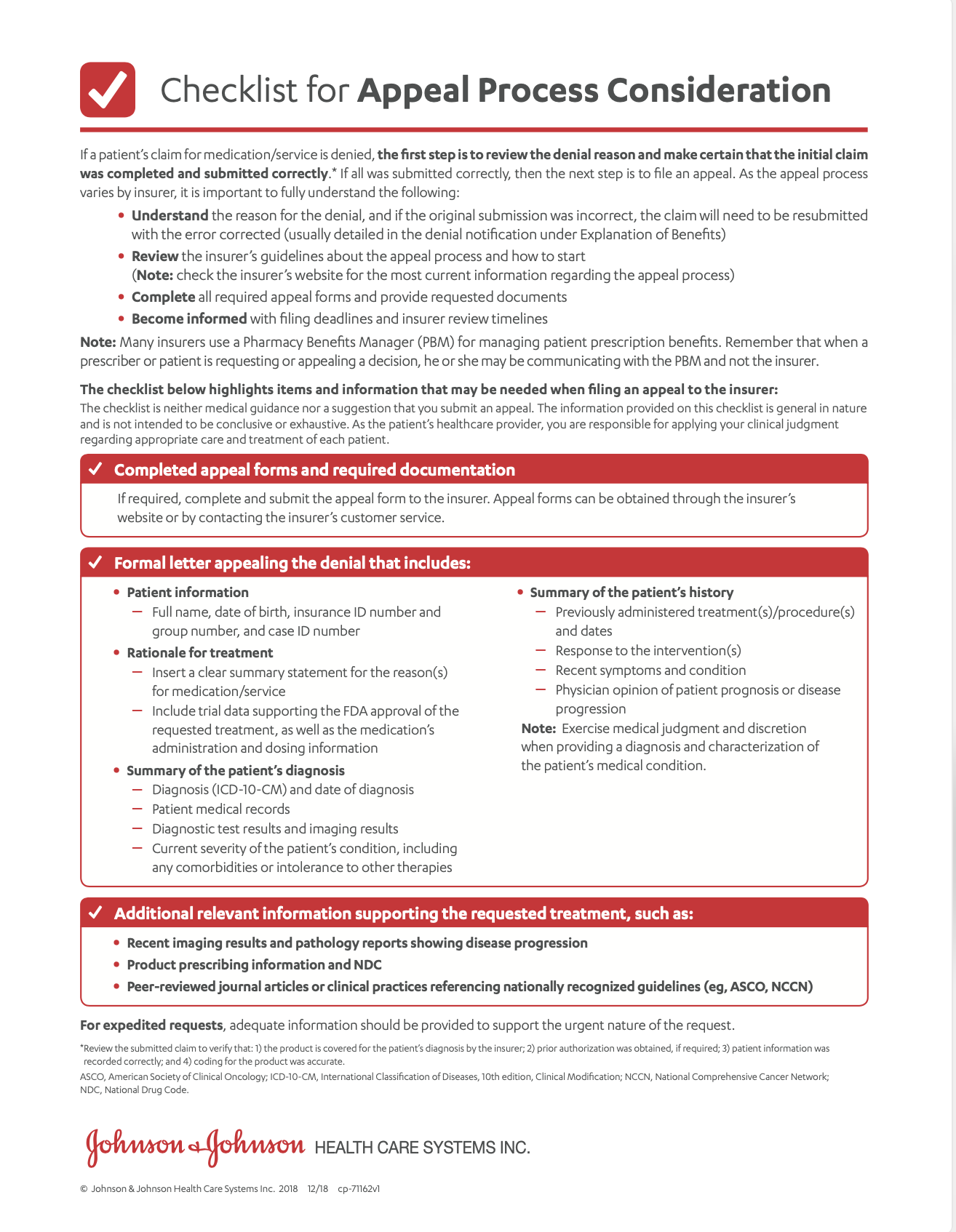
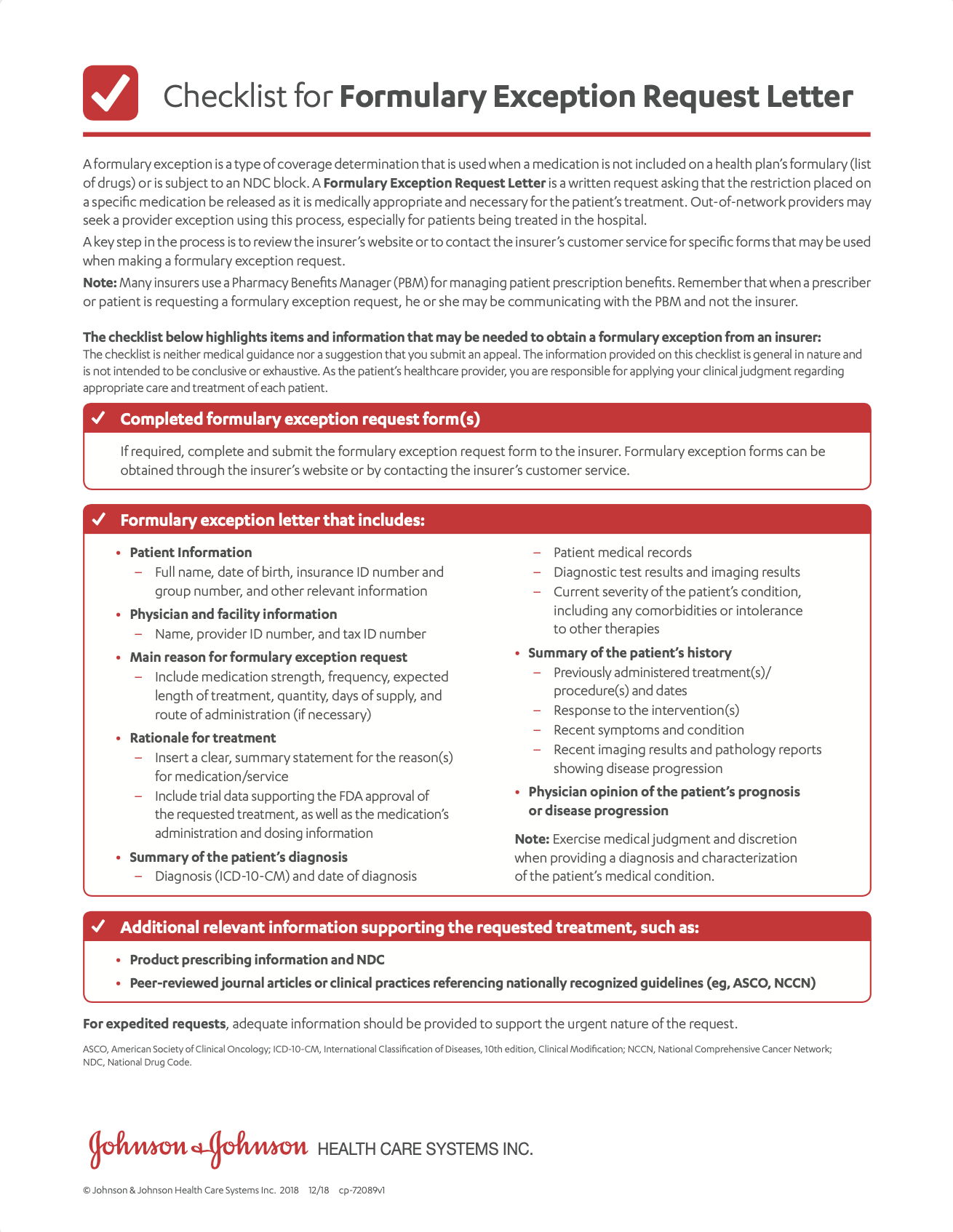
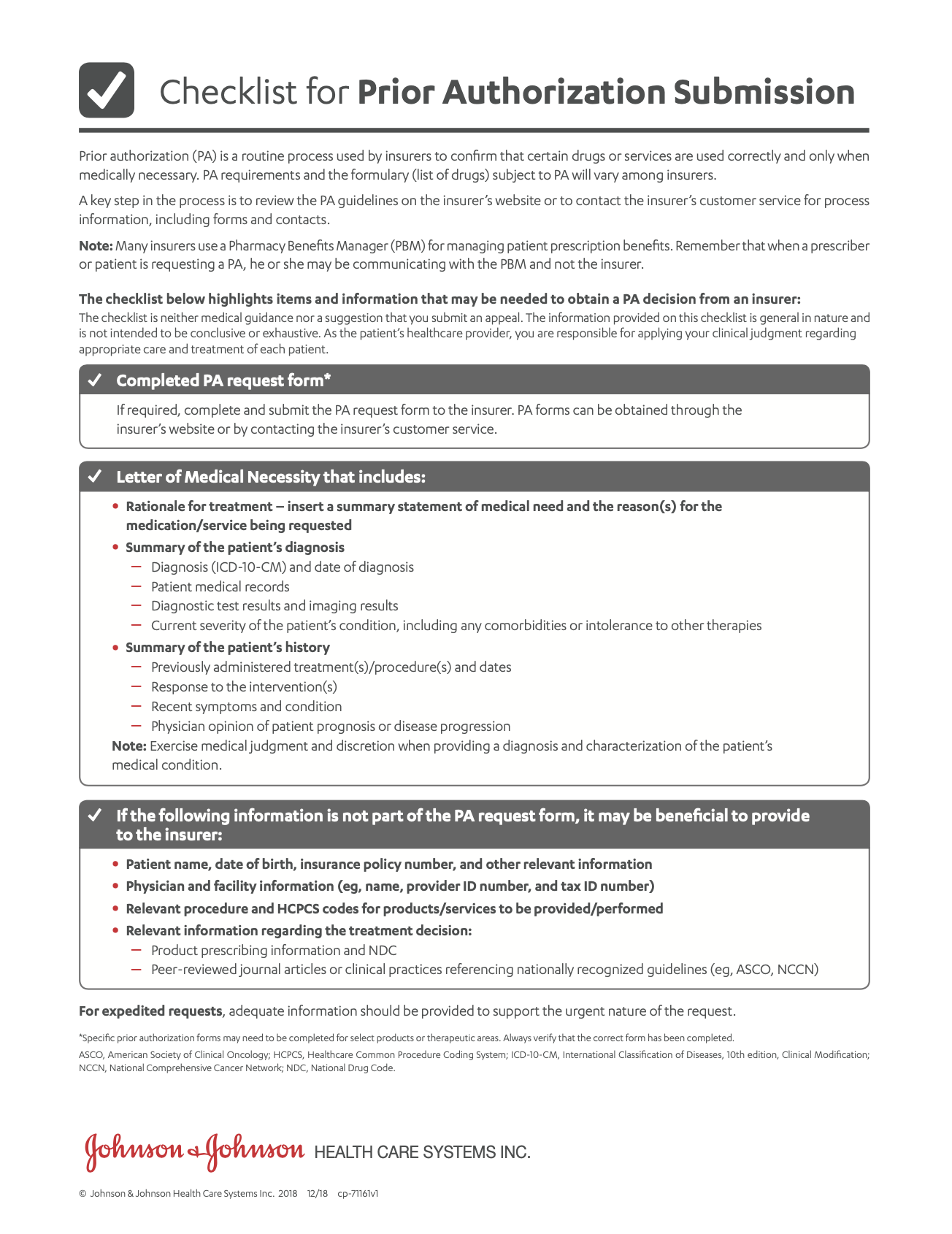
- Prior Authorization Tips
 A list of items and information that may be needed to obtain a coverage decision from an insurer.
A list of items and information that may be needed to obtain a coverage decision from an insurer. - Steps to Getting Your Medicine
 A patient-friendly guide to the verification and delivery process.
A patient-friendly guide to the verification and delivery process.
Steps to Getting Your Medicine (en español) - Steps to Getting Your Medicine (en español)A patient-friendly guide to the verification and delivery process.
- VELETRI® Prescription and Statement of Medical Necessity (PSMN)
 Complete and submit this form first to get your patient started on VELETRI®.
Complete and submit this form first to get your patient started on VELETRI®. - VELETRI® Prescription and Statement of Medical Necessity (PSMN)—For Veterans Affairs Patients OnlyComplete and submit this form first to get your Veterans Affairs patient started on VELETRI®.
X
Hover on a document on the left for a quick document preview
Welcome to Janssen CarePath


- Initiate Patient on VELETRI®
- Insurance Coverage
- Reimbursement
- Affordability
- Treatment Support
VELETRI® is marketed by Janssen Pharmaceuticals, Inc.